The Weight Regain Question
Perhaps no question about semaglutide generates more discussion than: "What happens when you stop?" The answer, supported by rigorous clinical trial data, has profound implications for how we understand and treat obesity. Data from the STEP 1 extension study and the STEP 4 trial demonstrate that weight regain after semaglutide discontinuation is substantial — but this finding actually reinforces an important medical principle [1].
STEP 1 Extension: One Year After Stopping
The STEP 1 extension study, published in Diabetes, Obesity and Metabolism in 2022 by Wilding et al., followed participants from the original STEP 1 trial for an additional year after treatment ended [1].
Study Design:
- Participants who completed the 68-week STEP 1 trial were followed for an additional 52 weeks off treatment (total 120 weeks)
- No semaglutide or placebo was administered during the extension period
- Lifestyle counseling continued
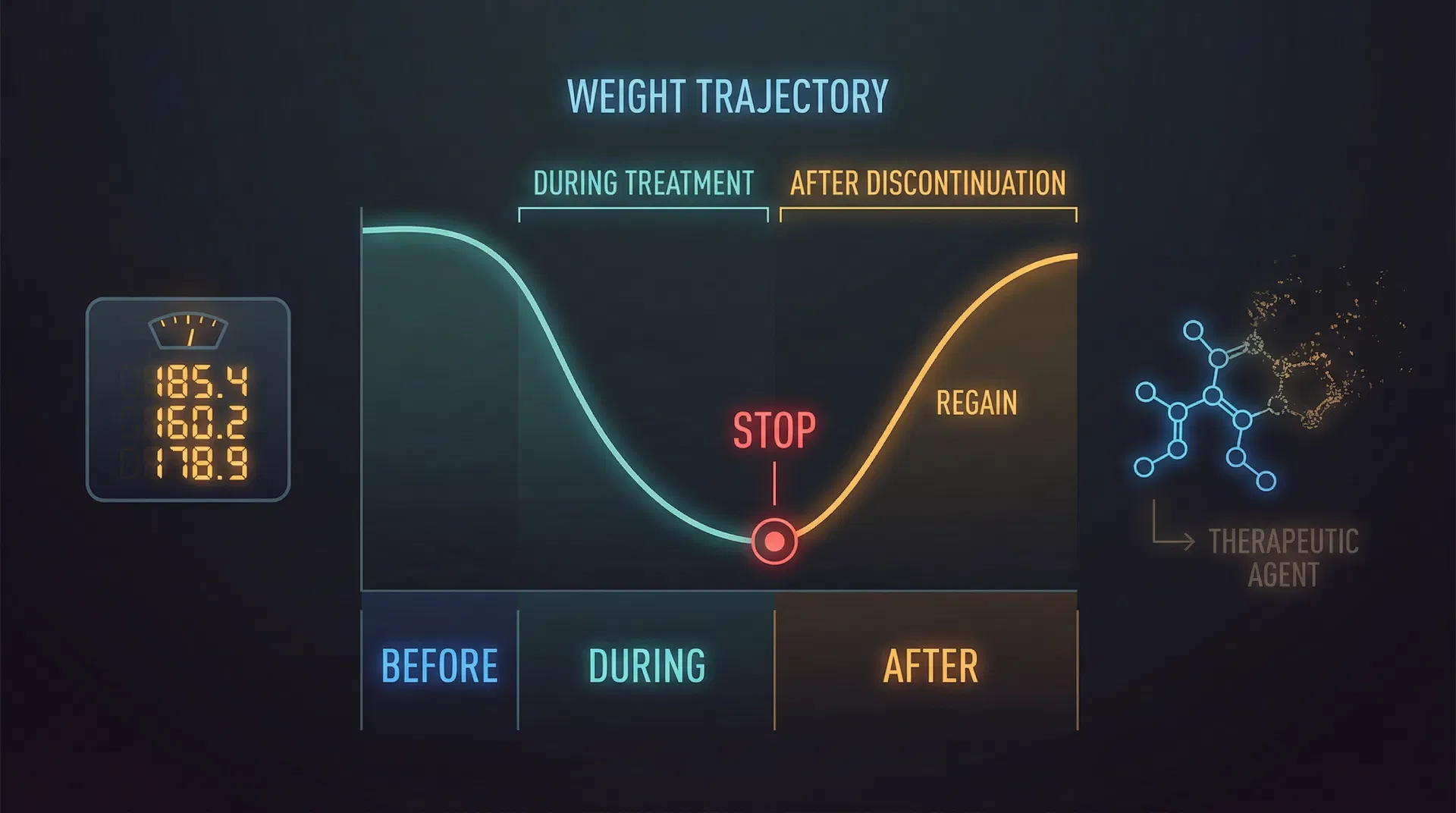
Weight Trajectory:
- End of treatment (week 68): Semaglutide group had lost -14.9% body weight
- One year after stopping (week 120): Semaglutide group had regained weight, with net loss of approximately -5.6% from original baseline
- Weight regained: Approximately two-thirds (66%) of the weight lost during treatment was regained within one year of stopping
Cardiometabolic Regression: The improvements in cardiometabolic parameters also partially reversed:
- Waist circumference: Partially regained
- Blood pressure: Returned toward baseline
- Lipid improvements: Partially lost
- CRP (inflammation): Increased back toward pre-treatment levels
- HbA1c: Returned toward baseline
However, even one year after stopping, the former semaglutide group still maintained some residual benefit compared to their pre-treatment baseline [1].
Looking for a physician-guided approach? Telegenix connects you with licensed providers who specialize in peptide and testosterone optimization. Every protocol is built on your bloodwork. Learn more and book a consultation.
STEP 4: The Withdrawal Design
The STEP 4 trial, published in JAMA in 2021 by Rubino et al., used a clever withdrawal design to specifically study the effects of continuing vs. stopping semaglutide [2].
Study Design:
- Run-in phase (weeks 0-20): All 803 participants received semaglutide 2.4 mg (open-label)
- Randomization (week 20): Participants who completed run-in were randomized 2:1 to continue semaglutide or switch to placebo for 48 additional weeks
- This design isolated the effect of treatment withdrawal after initial weight loss
Results:
- During run-in (weeks 0-20): All participants lost approximately -10.6% body weight
- Continued semaglutide (weeks 20-68): Further lost to reach -17.4% total weight loss
- Switched to placebo (weeks 20-68): Regained weight, ending at -5.0% from original baseline
The Divergence:
- Treatment difference at week 68: -12.4 percentage points (P<0.001)
- Those who continued semaglutide lost an additional -7.9% body weight
- Those who switched to placebo regained +6.9% body weight
- The two groups diverged dramatically after randomization, creating a clear "scissors" pattern on the weight trajectory graph [2].
Why Does Weight Regain Occur?
Understanding weight regain requires understanding the biology of obesity:
Metabolic Adaptation:
- Weight loss triggers compensatory metabolic changes: reduced resting metabolic rate, increased hunger hormones (ghrelin), and decreased satiety hormones
- These adaptations evolved to protect against starvation and persist long after weight loss
- Semaglutide counteracts these adaptations while being taken, but the adaptations reassert themselves when the drug is stopped
Neurobiological Reset:
- Semaglutide acts on brain appetite centers to reduce hunger and increase satiety
- When the drug is removed, the brain's appetite regulation returns to its pre-treatment set point
- This is analogous to blood pressure rising when antihypertensive medication is stopped
The Set Point Theory:
- The body appears to defend a biological "set point" weight
- Semaglutide can shift this set point downward while active
- Discontinuation allows the set point to drift back toward its original level [3].
The Chronic Disease Model
The weight regain data has been instrumental in shifting the medical community's understanding of obesity:
Obesity as a Chronic Disease:
- Just as hypertension requires ongoing medication, obesity requires ongoing treatment
- Stopping semaglutide is analogous to stopping a blood pressure medication — the underlying condition returns
- This is not a "failure" of the drug but rather confirmation that obesity is a chronic, relapsing condition
Treatment Duration:
- Current evidence supports indefinite treatment for patients who respond to semaglutide
- The STEP 5 trial showed sustained efficacy over 2 years with continued treatment
- There is no evidence of tolerance (needing higher doses over time) developing
Insurance and Policy Implications:
- Weight regain data supports the argument for long-term insurance coverage of anti-obesity medications
- Treating obesity as a chronic disease requiring ongoing pharmacotherapy aligns with how we treat other chronic conditions
Strategies to Mitigate Weight Regain
For patients who must discontinue semaglutide, several strategies may help mitigate weight regain:
- Gradual dose reduction: Tapering rather than abrupt discontinuation may ease the transition
- Intensive lifestyle intervention: Increased focus on diet and exercise during and after discontinuation
- Alternative medications: Switching to another weight management medication (e.g., phentermine-topiramate, naltrexone-bupropion) may help maintain some weight loss
- Behavioral support: Ongoing counseling and support groups
- Metabolic monitoring: Regular monitoring of weight and metabolic parameters to catch early regain
What Patients Should Know
For individuals considering or currently taking semaglutide:
- Plan for long-term use: If semaglutide is effective, plan to continue it indefinitely
- Weight regain is not your fault: It reflects biology, not willpower
- Some benefit persists: Even after stopping, some residual weight loss and metabolic benefit may remain
- Discuss with your doctor: Decisions about starting, continuing, or stopping should be made collaboratively with your healthcare provider
Related Comparison: [Ozempic vs Mounjaro: Complete Comparison](/compare/ozempic-vs-mounjaro)
References
-
Wilding JPH, Batterham RL, Davies M, et al. "Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension." Diabetes, Obesity and Metabolism. 2022;24(8):1553-1564. PubMed: 35441470
-
Rubino D, Abrahamsson N, Davies M, et al. "Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial." JAMA. 2021;325(14):1414-1425. PubMed: 33755728
-
Bergmann NC, Davies MJ, Lingvay I, Knop FK. "Semaglutide for the treatment of overweight and obesity: A review." Diabetes, Obesity and Metabolism. 2023;25(1):18-35. PMC: 10092086
Want to explore this therapy under medical supervision? Telegenix offers telehealth consultations with providers who specialize in peptides and hormone optimization. Book your free consultation today.
Related Reading
Explore more in-depth guides on related topics:
- STEP 1 Trial: How Semaglutide 2.4mg Achieved 15% Weight Loss in Adults
- [SURMOUNT-4 Trial: What Happens When You Stop Tirzepatide — The Weight Regain Data](/library/tirzepatide-surmount-4-stopping-weight-regain)
- Semaglutide: What the Science Actually Says — A PubMed-Backed Review
- STEP 5 Trial: Two-Year Semaglutide Data Proves Long-Term Weight Loss Durability
- SELECT Trial: Semaglutide Reduces Heart Attack and Stroke Risk by 20%
For a comprehensive overview, see our Complete Guide to Peptide Therapy.