As men age, a natural decline in testosterone levels is an inevitable physiological process. After the age of 30, testosterone levels typically decrease by approximately 1-2% per year. By the time men reach their 40s, this gradual reduction can accumulate, leading to a noticeable impact on their quality of life. Many men in this age group begin to experience a constellation of symptoms that can range from subtle to significantly disruptive. The challenge lies in distinguishing between the normal, age-related changes that are part of the aging process and a medical condition known as hypogonadism, which may warrant therapeutic intervention.
This comprehensive guide is designed to empower men over 40 with the knowledge to understand the evidence surrounding age-related testosterone decline, recognize potential symptoms, navigate the diagnostic process, and make informed decisions about whether Testosterone Replacement Therapy (TRT) is a suitable option for them. We will explore the nuances of testosterone physiology, the diagnostic criteria for low testosterone, various treatment modalities, and crucial considerations for men embarking on TRT in their fifth decade and beyond.
Understanding Age-Related Testosterone Decline
Testosterone is the primary male sex hormone, playing a crucial role in maintaining muscle mass, bone density, red blood cell production, libido, energy levels, and cognitive function. The normal range for total testosterone in adult men is generally considered to be 300-1000 nanograms per deciliter (ng/dL). However, this is a broad range, and individual optimal levels can vary significantly.
It's important to differentiate between total testosterone and free testosterone. Total testosterone measures all the testosterone in your blood, including that which is bound to proteins. The vast majority of testosterone (about 98%) is bound to two proteins: Sex Hormone Binding Globulin (SHBG) and albumin. Only a small percentage (1-2%) circulates as free testosterone, which is the biologically active form that can readily enter cells and exert its effects.
As men age, not only does total testosterone tend to decline, but Sex Hormone Binding Globulin (SHBG) levels often increase. This increase in SHBG can further reduce the amount of free, bioavailable testosterone, even if total testosterone levels appear to be within the "normal" range. This is why symptoms often matter more than just a single total testosterone number. A man with a total testosterone of 400 ng/dL might feel perfectly fine if his SHBG is low, leading to adequate free testosterone. Conversely, a man with the same total testosterone but high SHBG could experience significant symptoms due to low free testosterone.
Data from longitudinal studies, such as the Baltimore Longitudinal Study of Aging, have consistently shown a progressive decline in total and free testosterone levels with increasing age [PMID: 15601955]. This decline is not necessarily indicative of a disease state in all men, but for many, it crosses a threshold where symptoms become clinically significant.
Symptoms That May Indicate Low Testosterone
The symptoms of low testosterone (hypogonadism) are often non-specific and can overlap with many other medical conditions or simply be attributed to the normal aging process. This makes accurate diagnosis challenging but highlights the importance of thorough evaluation. If you are a man over 40 experiencing several of the following, it may be worth discussing with your healthcare provider:
- Fatigue and low energy: Persistent tiredness, even after adequate sleep, and a general lack of motivation. [Fatigue & low testosterone]
- Decreased libido: A noticeable reduction in sexual desire or interest.
- Erectile dysfunction (ED): Difficulty achieving or maintaining an erection. [Erectile dysfunction options]
- Loss of muscle mass and strength: Despite maintaining a consistent exercise routine, a noticeable decrease in muscle bulk and strength.
- Increased body fat, especially visceral fat: An increase in abdominal fat, often referred to as a "beer belly," which is linked to metabolic syndrome.
- Brain fog and poor concentration: Difficulty focusing, memory issues, and a general feeling of mental sluggishness.
- Mood changes and irritability: Increased irritability, anxiety, depression, or a general feeling of being "down." [Depression & testosterone]
- Poor sleep quality: Insomnia, restless sleep, or waking up feeling unrefreshed.
- Decreased bone density: Though often asymptomatic until a fracture occurs, low testosterone contributes to osteoporosis.
It is crucial to remember that these symptoms can also be caused by stress, poor diet, lack of exercise, sleep disorders, thyroid issues, depression, diabetes, and other medical conditions. Therefore, a comprehensive medical evaluation is essential to rule out other causes before attributing them solely to low testosterone.
Getting Tested: What Bloodwork to Request
If you suspect low testosterone based on your symptoms, the next step is to get comprehensive bloodwork. Proper testing is critical for an accurate diagnosis.
Here's a list of essential blood tests to request:
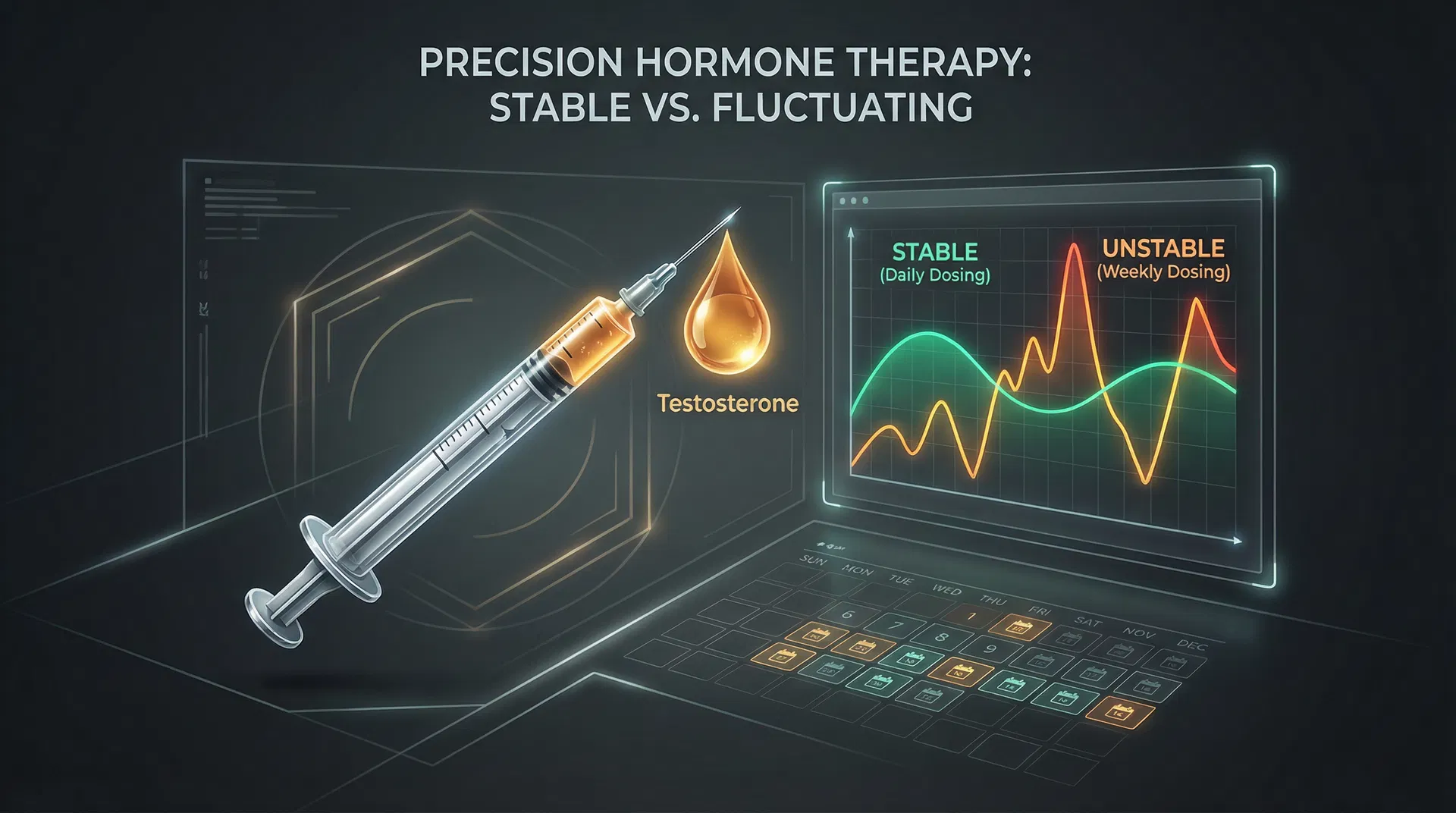
- Total Testosterone: This is the initial screening test. It is crucial to have this drawn in the morning, ideally between 7:00 AM and 10:00 AM, as testosterone levels are highest at this time and decline throughout the day.
- Free Testosterone: This measures the unbound, biologically active testosterone. Given the age-related increase in SHBG, free testosterone is often a more accurate indicator of bioavailable testosterone levels in older men.
- Sex Hormone Binding Globulin (SHBG): This protein binds to testosterone, making it unavailable to tissues. Knowing your SHBG level helps interpret total and free testosterone results.
- Estradiol (E2): Testosterone can be converted into estrogen (estradiol) by the aromatase enzyme. High estradiol levels in men can contribute to symptoms like gynecomastia, fluid retention, and mood changes.
- Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH): These pituitary hormones regulate testosterone production in the testes. High LH/FSH with low testosterone indicates primary hypogonadism (problem with the testes), while low LH/FSH with low testosterone indicates secondary hypogonadism (problem with the pituitary or hypothalamus).
- Complete Blood Count (CBC): To check red blood cell count (TRT can increase hematocrit), white blood cell count, and platelet count.
- Prostate-Specific Antigen (PSA): Essential for prostate health monitoring, especially in men over 40 before and during TRT.
- Lipid Panel: To assess cholesterol and triglyceride levels, as TRT can sometimes affect lipid profiles.
- Comprehensive Metabolic Panel (CMP): To assess kidney function, liver function, electrolytes, and blood glucose.
- Thyroid Panel (TSH, Free T3, Free T4): To rule out thyroid dysfunction, which can mimic many symptoms of low testosterone.
Important Note on Diagnosis: The Endocrine Society guidelines recommend two separate morning blood draws showing consistently low testosterone levels, along with classical symptoms, before a diagnosis of hypogonadism is made and TRT is considered. This helps account for day-to-day fluctuations in hormone levels. [Bloodwork guide]
When TRT Is Appropriate: The Clinical Criteria
The decision to initiate TRT is a significant one and should be based on a combination of clinical symptoms and laboratory findings. The Endocrine Society guidelines (2018) provide a framework for diagnosis and treatment:
TRT is generally considered appropriate for men with symptoms consistent with hypogonadism PLUS consistently low testosterone levels (typically defined as total testosterone below 300 ng/dL on at least two separate morning measurements, or consistently low free testosterone).
The "Gray Zone" (300-400 ng/dL): This is where clinical judgment becomes paramount. Men in this range may or may not experience symptoms. If symptoms are significant and other causes have been ruled out, a trial of TRT might be considered, with careful monitoring of symptom improvement and side effects. Some clinicians use free testosterone as a more definitive guide in this range. For men in this gray zone, lifestyle modifications (diet, exercise, sleep, stress reduction) should always be prioritized first.
Contraindications to TRT: Certain medical conditions make TRT inappropriate or require extreme caution:
- Active prostate cancer or breast cancer: TRT is generally contraindicated in men with these conditions due to concerns about stimulating cancer growth.
- Untreated severe sleep apnea: TRT can exacerbate sleep apnea. This condition should be managed before initiating TRT.
- Uncontrolled heart failure (NYHA Class III or IV): TRT may worsen fluid retention in these patients.
- Severe lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) that are untreated: TRT can potentially worsen LUTS.
- Hematocrit >50%: High red blood cell count can increase the risk of blood clots. This needs to be managed before TRT.
- Desire for near-term fertility: TRT suppresses natural sperm production and can lead to infertility. Men desiring fertility should explore alternatives like Clomiphene or HCG. [TRT and fertility]